This study aimed to document the prevalence of active trachoma and trichiasis from 1997 to 2003 and from 1987 to 2004, respectively, and to provide an overview of trachoma control activities in Australia in 2004. Prevalence data were obtained from state, territory and regional population health units and unpublished surveys. Information about trachoma control programs and activities currently implemented in Australia was obtained through structured interviews with staff involved in trachoma control. Active trachoma prevalences in Aboriginal and Torres Strait Islander children, ranging from 0–40 per cent, were reported from the Eastern Goldfields, Midwest-Murchison and Kimberley Population Health Units in Western Australia and the Northern Territory’s Centre for Disease Control. Large differences in trachoma prevalence were reported within and between different regions and from different years in the same region. Recent surveys of trichiasis in Kimberley and Central Australian Aboriginal and Torres Strait Islander adults demonstrated prevalences of 9–12 per cent in inland, desert areas. In contrast with developing countries where active trachoma and trichiasis are more common among adult women than men, Australian surveys have identified equal prevalence in both sexes. Interpretation of trachoma prevalence and inter-regional/state/national comparisons were hampered by lack of a uniform method of data collection and analysis. Trachoma control programs were implemented consistently in some communities, and irregularly and/or in piecemeal fashion in others. Trachoma control programs led by regional population health units working in collaboration with primary health care services were more likely to be consistently implemented over long periods of time. Trachoma is a significant public health issue in some Aboriginal communities within Australia. The Communicable Diseases Network Australia has developed guidelines for the public health management of trachoma which provide recommendations on trachoma screening, control and data collection trachoma for affected states and territories. Commun Dis Intell 2006;30:236–247.
Top of page
Introduction
Trachoma is caused by Chlamydia trachomatis infection of the conjunctiva. Recurrent infection may result in conjunctival scarring, trichiasis, corneal opacification and blindness. Although trachoma had disappeared from most parts of remote Australia by the 1930s as housing, hygiene and living conditions improved, active trachoma in Aboriginal and Torres Strait Islander children, and trichiasis in Aboriginal and Torres Strait Islander adults, is still found in some regions.1
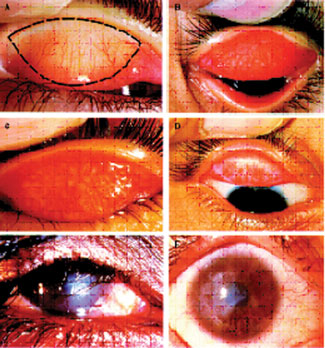
The World Health Organization (WHO) trachoma grading system and ‘SAFE’ intervention strategy have been implemented in some trachoma-endemic areas of Australia for many years.2,3,4 The WHO simplified trachoma grading system classifies trachoma into five clinical stages: follicular trachomatous inflammation (TF); intense trachomatous inflammation (TI); trachomatous scarring (TS); trachomatous trichiasis (TT); and corneal opacity (CO) as shown in the Figure.2 The SAFE acronym stands for Surgery for trichiasis, community use of Antibiotics to reduce transmission of chlamydial infection, Facial cleanliness, and Environmental health improvements.4 The WHO recommends that active trachoma (i.e. TF and/or TI) prevalence in children aged 1–10 years be used to determine the nature and coverage of public health interventions for trachoma within a community or population.2 The WHO and its partners (including Australia) aim to eliminate avoidable blindness, including blinding trachoma, (VISION 2020 – the right to sight) by 2020.5
Figure. World Health Organization simplified trachoma grading classification system2
Prevalence data for active trachoma until 1996, and for trichiasis until 1980, in many trachoma-endemic regions have already been published.6,7,8 This paper aimed to document the prevalence of active trachoma and trichiasis from 1997 to 2003 and from 1987 to 2004, respectively, and to provide an overview of trachoma control activities in Australia in 2004.
Top of page
Methods
Active trachoma and trichiasis prevalence
In June 2003, the Office for Aboriginal and Torres Strait Islander Health (OATSIH), a division of the Australian Government Department of Health and Ageing (DoHA), requested prevalence data on active trachoma in children collected after 1987, and on trichiasis in adults collected after 1980, from the Northern Territory, Queensland, New South Wales, South Australian and Western Australian health departments. Tasmania, Victoria and the Australian Capital Territory were not surveyed as trachoma had ceased to be a public health problem in these jurisdictions decades ago. Data were collected using a WHO survey proforma. If prevalence data for individual communities were reported, these were combined into regional datasets based on Australian Bureau of Statistics (ABS) census collection regions due to the small populations of many Aboriginal and Torres Strait Islander communities. Trachoma prevalent areas, whilst large geographically, are remote and sparsely populated.
Regional population data were obtained from the ABS Census of Population and Housing, or in the case of some regions in Western Australia, from the Western Australian Department of Education or the Western Australia Department of Health. It was not always possible to match population estimates with the age range screened. Where this was not possible the closest age range estimates are given. The regional population data presented are for Aboriginal and Torres Strait Islander children only, with the exception of the Murchison region of Western Australia where non- Aboriginal and Torres Strait Islander children were included.
Trachoma control programs
Information about trachoma control programs and activities currently implemented in Australia was obtained through structured interviews with 95 people conducted by DBM between July and August 2004. Interviewees included people involved in trachoma or communicable disease control at state, territory and regional population health unit and primary health care levels, and ophthalmologists and optometrists.
Interviews lasted 20 to 60 minutes depending on the interviewee’s level of involvement in trachoma control programs/activities. Where available, trachoma control guidelines, staff education resources and reports of trachoma control activities were obtained from interviewees.
Top of page
Results
Active trachoma prevalence in children, 1997–2003
The data presented in Table 1 were reported by the Eastern Goldfields, Midwest-Murchison and Kimberley Population Health Units of the Department of Health Western Australia and the Northern Territory Government’s Centre for Disease Control.
Table 1. Active trachoma prevalence in Australia, 1997–2003*
Location |
Age group surveyed |
Month and year of survey |
Estimated number of Indigenous children in region† |
Number of children examined for active trachoma |
Number of children examined with active trachoma |
Active trachoma prevalence in children examined
(%) |
NT |
| Barkly |
5–15 |
2002 |
810§§,11 |
81 |
10 |
12 |
| Barkly |
5–15 |
2001 |
810§§,11 |
90 |
3 |
3 |
| Barkly |
5–15 |
1998 |
925§§,12 |
60 |
3 |
5 |
| Barkly |
5–15 |
1997 |
925§§,12 |
237 |
14 |
6 |
| East Arnhem |
5–15 |
2002 |
1,816§§,11 |
675 |
135 |
20 |
| East Arnhem |
5–15 |
2001 |
1,816§§,11 |
143 |
0 |
0 |
| East Arnhem |
5–15 |
1998 |
1,828§§,12 |
93 |
3 |
3 |
| Katherine |
5–15 |
2002 |
1,850§§,11 |
344 |
3 |
1 |
| Katherine |
5–15 |
2001 |
1,850§§,11 |
231 |
7 |
3 |
| Katherine |
5–15 |
2000 |
1,829§§,11 |
623 |
142 |
23 |
| Katherine |
5–15 |
1999 |
1,829§§,12 |
420 |
67 |
16 |
| Katherine |
5–15 |
1998 |
1,829§§,12 |
223 |
35 |
16 |
| Katherine |
5–15 |
1997 |
1,829§§,12 |
329 |
35 |
11 |
| Darwin Rural |
5–15 |
2002 |
2,270§§,11 |
347 |
30 |
8 |
| Darwin Rural |
5–15 |
2001 |
2,270§§,11 |
569 |
6 |
1 |
| Darwin Rural |
5–15 |
2000 |
2,079§§,11 |
513 |
15 |
3 |
| Darwin Rural |
5–15 |
1999 |
2,079§§,12 |
639 |
37 |
6 |
| Darwin Rural |
5–15 |
1998 |
2,079§§,12 |
336 |
53 |
16 |
| Alice Springs |
5–15 |
Jun 1999 |
2,789§§,12 |
278 |
97 |
35 |
| Alice Springs |
5–15 |
1998 |
2,789§§,12 |
119 |
47 |
40 |
WA |
| Eastern Goldfields |
<18‡ |
May-June 2003 |
>2,028§,9 |
516 |
140|| |
27 |
| Murchison¶ |
1–10 |
March 2002 |
304** |
129** |
34 |
26 |
266†† |
82†† |
3 |
4 |
| Murchison¶ |
1–10 |
March 2001 |
304** |
146** |
14 |
10 |
266†† |
92†† |
7 |
8 |
| Murchison¶ |
1–10 |
March 2000 |
304** |
126** |
16 |
13 |
266†† |
92†† |
0 |
0 |
| Murchison¶ |
1–10 |
March 1999 |
304** |
137** |
10 |
7 |
266†† |
129†† |
0 |
0 |
| Murchison¶ |
1–10 |
March 1998 |
304** |
127** |
13 |
10 |
266†† |
105†† |
2 |
2 |
| Murchison¶ |
1–10 |
March 1997 |
304** |
190** |
41 |
22 |
266†† |
131†† |
1 |
1 |
| Kimberley‡‡ |
5–16+ |
Sept-Nov 2002 |
3,63910 |
1,670 |
178 |
11 |
| Kimberley‡‡ |
5–16+ |
Sept-Nov 2001 |
3,69310 |
1,676 |
195 |
12 |
Top of page
Queensland Health reported minimal trachoma data collected through laboratory notifications. Active trachoma prevalence could not be ascertained from these data.
South Australian health authorities reported verbally that they had no data on trachoma. No response was received from NSW Department of Health.
As shown in Table 1, there was considerable variation in sampling methods, and in the proportion of the regional childhood population examined for active trachoma between different regions. Large differences in active trachoma prevalence between regions and in the same region between different years were observed. In addition (not shown in Table 1), there were large differences in active trachoma prevalence between towns and communities within the same region. For example, in the Kimberley in 2003 regional active trachoma prevalence was reported as 11 per cent. Trachoma is no longer endemic in some Kimberley towns and coastal communities, which therefore were not screened, and trachoma prevalence in screened schools and communities ranged from 5 per cent to 60 per cent.13 Apart from the Eastern Goldfields where a small proportion of TI was reported, TF and TI prevalences were not reported separately.
Data on the Aboriginal and/or Torres Strait Islander status of children examined were not reported, except from the Murchison region.
Trichiasis prevalence in adults, 1987 to 2004
No trichiasis data were available for 1981 to 1986. From 1987 to 2004, survey data on trichiasis prevalence were available from only the Kimberley, Central Australia and the Anangu Pitjantjatjara lands, as shown in Table 2. As with active trachoma, there were marked differences in trichiasis prevalence both between and within regions. No differences in trichiasis prevalence between men and women were observed.
Table 2. Trichiasis prevalence in Australia, 1987 to 2004
Location |
Year |
Population screened |
Percentage of target population screened |
Trichiasis prevalence
(%) |
WA |
| Kimberley (excluding Broome Shire)14 |
2004 |
Aboriginal and Torres Strait Islander 50+ years |
20.0* |
9.5†
(Halls Creek Shire 12.5, Wyndham-East Kimberley Shire 6.0, Derby – West Kimberley Shire 4.3) |
| Kimberley7 |
1998 |
Aboriginal and Torres Strait Islander 50+ years |
41.8‡ |
2.9†
(Halls Creek Shire 11.0, Wyndham-East Kimberley Shire 1.8, Derby – West Kimberley Shire 1.7
Broome Shire 1.0) |
| Fitzroy Crossing15 |
1993 |
Not reported |
Not reported |
1.0 |
NT |
| Central Australia16 |
2003 |
Aboriginal and Torres Strait Islander 40+ years, presenting to a general ophthalmology outreach clinic for symptoms/reasons unrelated to trachoma |
100% |
9.0† |
| Alice Springs/Barkly17 |
1987-90 |
Aboriginal and Torres Strait Islander, 40+ years |
Not reported |
5.2 |
| Katherine17 |
1987-90 |
Aboriginal and Torres Strait Islander, 40+ years |
Not reported, <30 people screened |
6.9 |
| Darwin Rural17 |
1987-88 |
Aboriginal and Torres Strait Islander, 40+ years |
Not reported, <30 people screened |
0 |
| East Arnhem17 |
1987-89 |
Aboriginal and Torres Strait Islander, 40+ years |
Not reported |
13.0 |
SA |
| A-P§ lands18 |
1999-2000 |
Aboriginal and Torres Strait Islander, all ages |
75% |
0.6 (5.2% in 50 + years age group) |
| A-P lands19 |
1989-90 |
Aboriginal and Torres Strait Islander, all ages |
54.3% |
2.9 (19.1% in 60+ years age group) |
Top of page
In the Kimberley region, trichiasis prevalence was significantly higher in inland, desert areas than in those in close proximity to the sea or major rivers.7,14 A survey by Landers, et al in 2003 indicated that trichiasis was still endemic among Aboriginal and Torres Strait Islander adults in Central Australia.16 Many health professionals reported rarely or never seeing trichiasis but no recent data were available from areas outside the Kimberley and Central Australia.
Trachoma control
Notification of trachoma
Trachoma is not a nationally notifiable disease based on clinical diagnosis nor through laboratory notifications. It is also not notifiable based on clinical diagnosis in any State or Territory, except in Western Australia where notification has not been requested since 1993 because local experience demonstrated that it was neither an appropriate nor an effective surveillance strategy. In Queensland and the Northern Territory, laboratory notifications of Chlamydia trachomatis specify the site from which the isolate was obtained. This allows differentiation between ocular and genital Chlamydia infections but does not distinguish trachoma from C. trachomatis genital serovar ocular infections (i.e. inclusion conjunctivitis and paratrachoma).
Trachoma control programs/activities
Australian and WHO trachoma guidelines identified by this study are summarised in Table 3. The Northern Territory and several Western Australian regions had trachoma control programs and trachoma control guidelines. The Central Australian Remote Practitioners Association (CARPA) guidelines and Therapeutic Guidelines: Antibiotic were also used in clinical management of trachoma.22,24 Few practitioners reported knowledge or use of the OATSIH Specialist Eye Health Guidelines for use in Aboriginal and Torres Strait Islander Populations or those developed by Couzos and Taylor.21 All trachoma control guidelines commonly used in Australia are based on the 1993 WHO guidelines, and do not include changes recommended by the WHO in 2004.
Table 3. Comparison of the ‘A’, ‘F’ and ‘E’ components of the WHO and Australian trachoma control guidelines*
Source |
Screening target group |
Screening interval |
Screening time |
Consent process |
Recommended treatment/interventions |
Hyperendemic, prevalence >20% |
Endemic, prevalence 5–19% |
Non-endemic, prevalence <5% |
| WHO 1993†,2 |
Children 1–10 years |
Annual |
Not specified |
Not specified |
Topical antibiotic treatment to all community members
Systemic antibiotics to severe cases
Face-washing and environmental health improvement |
Topical antibiotic treatment to all community members or to cases and their families
Face-washing and environmental health improvement |
Topical antibiotic treatment for cases only |
| WHO 2003†,20 |
Children 1–9 years |
Every 3 years |
Not specified |
Not specified |
If prevalence ≥10%: annual antibiotic treatment of all community members aged >6 months until prevalence <5%, aim for 80% coverage of eligible population; hygiene promotion and environmental improvement to achieve 80% of children with clean faces |
|
If prevalence <10%: antibiotic treatment of cases and their families |
| OATSIH, Australia 2001‡,3 |
Children 2–7 years |
Not specified |
Not specified |
Not specified |
|
Azithromycin to cases and their family/household (i.e. people who live together or share a sleeping area), repeat treatment annually until active trachoma disappears
If prevalence >20%, it may be simpler to treat the entire community
Promote environmental health and facial cleanliness |
|
| Aboriginal primary health care 200321 |
Children 1–9 years |
Not specified |
Not specified |
Not specified |
|
As for OATSIH, above |
|
| Therapeutic guidelines: antibiotic 200322 |
– |
– |
– |
– |
Community-based treatment program using azithromycin |
Azithromycin to cases and their household contacts |
|
| Centre for Disease Control NT 1998†,23 |
School aged children in remote areas, as part of Healthy School Aged Kids Program |
Annual if trachoma prevalence >5% |
Not specified |
Written consent for screening
Verbal consent from individual caregivers for treatment |
Azithromycin to all children >6 months of age and their female care-givers within 14 days after screening and at six months
Health promotion |
Azithromycin to cases and their household contacts |
Azithromycin to cases only |
| CARPA 2003†,§,24 |
– |
– |
– |
– |
|
Azithromycin to cases and their household contacts within 14 days
Erythromycin twice daily for 14 days if <6 months
Check with local CDC for who else needs treatment
Encourage face and hand washing |
|
| Kimberley Population Health Unit WA 2004†,13 |
School aged children and household members of school aged children with TF |
Annual
Cease screening if prevalence <5% for 5 consecutive years |
Sept, Oct, Nov |
Varies from written individual consent to verbal community consent |
Azithromycin to all school children with TF and their household contacts aged 5–16 years, and to all children aged 1–4 years
Environmental health and health promotion |
Azithromycin to all school children with TF and their household contacts aged 1–16 years found to have trachoma
Environmental health and health promotion |
Azithromycin to all school children with TF and their household contacts aged 1–16 years found to have trachoma
Environmental health and health promotion |
| Pilbara Population Health Unit WA 2004†,25 |
School children
Children 6 months–5 years and school aged household members of children with >5 trachoma follicles or TI
Household members where more than 1 child has ≥1 trachoma follicle |
Annual if trachoma prevalence >5% |
June, July |
Written consent for screening and treatment of school aged children |
As for Kimberley Population Health Unit |
As for Kimberley Population Health Unit |
As for Kimberley Population Health Unit |
| Mid-West and Murchison Population Health Unit WA 2003†,27 |
As for Pilbara Population Health Unit |
Annual if trachoma prevalence >5% |
February, March – completed in one week |
Written consent for screening
Verbal consent from individual caregivers for treatment |
Azithromycin to all community members >6 kg
Environmental health and health promotion |
Azithromycin to children with TF and their family members.
Environmental health and health promotion |
| Goldfields Population Health Unit WA 2004†,27 |
As for Mid-West and Murchison Population Health Unit |
Annual if trachoma prevalence >5% |
May, completed in one week |
Community consent for screening
Verbal consent from individual caregivers for treatment |
As for Midwest Murchison Population Health Unit |
As for Midwest Murchison Population Health Unit |
Top of page
In the Northern Territory, trachoma control was incorporated into the school health program which targets children living in remote communities and includes immunisation and annual screening for trachoma and a variety of other medical conditions. The program did not apply in the capital or major towns. Population health staff provided support for program implementation at the request of primary health care staff. Implementation of the program occurred annually in some communities, and irregularly and/or in piecemeal fashion in others.
Despite the absence of a state-wide approach to trachoma control in Western Australia, trachoma control programs had been established in four regional population units since the late 1980s/early 1990s. Population health units assumed responsibility for clinical leadership (through the development and distribution of regional trachoma control program guidelines and the provision of staff education and resources for staff and community education) and coordinating a regional approach to program implementation. Primary health care staff were responsible for trachoma screening, treatment and community education. There was general consensus that a regional approach, led by the population health unit working in collaboration with primary health care services, was crucial to the success and sustainability of trachoma control. Within each region, trachoma control was implemented in school settings over a specific one week to two month period with the aim of reducing the pool of active infection by screening and treating as many people in as short a time period as possible to prevent reinfection from untreated individuals in neighbouring areas. Programs were scheduled to occur during, or as soon as possible before, the maximal fly breeding season and took into account logistical constraints such as school holidays/camps, cyclones, flooding and customary law.
No statewide, regional or local trachoma control programs were identified in Victoria, the Australian Capital Territory, Tasmania, Queensland, South Australia or New South Wales.
Since all trachoma control programs currently in operation in Australia target school aged children, there has been relatively little focus on blinding trachoma or the ‘S’ component of the SAFE strategy. Screening and treatment for trichiasis were systematically implemented only in the Kimberley region of Western Australia.
Top of page
Discussion
Transmission of active trachoma and occurrence of trichiasis in Aboriginal and Torres Strait Islander communities is still a reality in 21st century Australia. Large differences in trachoma prevalence were reported from different regions and from different times within the same region. In contrast with developing countries where active trachoma and trichiasis are more common among adult women than men, Australian surveys have identified equal prevalence in both sexes.3,7,14,16,28–30 There were no consistently implemented state or territory level trachoma control programs. Trachoma control programs led by regional population health units working in collaboration with primary health care services were more likely to be consistently implemented over long periods of time.
Although Table 1 reports regional active trachoma prevalence, lack of standardisation of numerators and denominators between different regions means that it cannot be assumed that these data accurately reflect active trachoma prevalence in children <10 years in all Aboriginal and Torres Strait Islander communities within these regions. Reasons for this include:
- In some regions non-Aboriginal and Torres Strait Islander children were included in the surveys and their results included in prevalence calculations. They usually contribute very few, if any cases to the numerator but were not included in the denominator (except where specified in the Murchison region of Western Australia). This may result in an overestimation of regional trachoma prevalence within Aboriginal and Torres Strait Islander populations.
- In most regions where trachoma is known to be endemic, large populations of Aboriginal and Torres Strait Islander people live in areas where trachoma is, or is believed to be, no longer endemic, e.g. Broome, Darwin and Alice Springs. These populations were not included in the denominator when calculating regional trachoma prevalence. This may result in overestimation of regional Aboriginal and Torres Strait Islander trachoma prevalence.
- Age groups targeted for screening tend to be school aged children, but are not uniform across regions. Thus prevalence calculations may include data from children aged less than 10 years, while children aged one to four years are likely to be under-represented, if represented at all.
- Screening coverage of the target populations is generally low, so observed prevalence may not truly reflect population prevalence. For example screening coverage was 65 per cent, 67 per cent and 63 per cent in 1999, 2000 and 2001 respectively in the Kimberley, 71 per cent and 77 per cent in 1995 and 1996 respectively in the Katherine region, and 24 per cent in Central Australia in 1998, 1999 and 2000.31–34
A similar lack of standardisation of survey methods and prevalence calculations also applies to trichiasis data.
Some health professionals suggest that trachoma is no longer as prevalent or severe as previously in many regions and that trachoma may be over diagnosed in Australia. This may be attributed to the fact that clinical signs of active trachoma are not specific to trachoma, genital Chlamydia is highly endemic in many trachoma-endemic areas and may be present in ocular swabs,35 and trichiasis appears to be absent from some trachoma-endemic communities. However, a recent Northern Territory study identified C. trachomatis isolates corresponding to serovars Ba and C (i.e. trachoma, not genital, serovars) from ocular swabs.36 Genotyping of ocular swabs from Kimberley children presenting with conjunctivitis also confirmed the presence of C. trachomatis serovars Ba and C (personal communication, Drs Michelle Porter and David Smith, PathWest). Furthermore, recent trichiasis prevalence surveys indicate that trichiasis is still present in Central Australia and parts of the Kimberley region.7,14,16,18
Throughout Australia there is anecdotal, but no published, evidence that TI and TS are decreasing, indicating that trachoma may be decreasing in intensity and therefore less likely to result in trichiasis in later life.8 Thus, TI and TT prevalence data should be collected as a routine component of trachoma control.
National guidelines for the public health management of trachoma have been developed by the Communicable Disease Network Australia (Box).37 These guidelines are consistent with the spirit of, but do not replicate, the WHO guidelines because high level evidence from randomised controlled trials or meta-analyses of randomised controlled trials exists only for the ‘S’ component of the SAFE strategy, and because it was considered important that Australian guidelines reflect Australian experiences of trachoma control.28,38,39,40 As described in this paper, there is considerable trachoma control activity underway within Australia. The new Australian guidelines will promote consistent trachoma screening and control programs, and result in a strengthened national collaboration in surveillance and data collection.
Top of page
Box. Key recommendations from Guidelines for the public health management of trachoma37
|
Recommendation |
| |
Trachoma control should be the responsibility of government-run regional population health units and be organised on a regional basis where population mobility is high. Primary health care services should be involved in the detection and treatment of trachoma under the coordination of population health units. |
| |
Trachoma control activities should be planned and implemented in consultation with community representatives and other key stakeholders. |
| |
Areas with the highest number of persons with active trachoma and areas with the highest prevalence of active trachoma should be prioritised for trachoma control. |
| |
Regional population health units should collect trachoma data in accordance with the minimum national trachoma dataset. |
| Surgery |
Regional population health units, primary health care services and specialist eye health services need to decide, collaboratively, on the best way of identifying patients with trichiasis in their region and the best system to ensure that these patients have access to timely surgical referral and treatment. |
| |
In regions where trachoma is endemic but trichiasis prevalence is unknown, the burden of trichiasis should be quantified. |
| |
In areas where trachoma or trichiasis is or has been endemic, Aboriginal and Torres Strait Islander people aged 40–54 years should be screened every two years and those aged 55+ years should be screened annually for trichiasis as part of an adult health check |
| |
Patients with trichiasis should be referred to an ophthalmologist for surgical intervention. |
| |
Following trichiasis surgery, patients should be followed up annually so that recurrences can be detected promptly |
| Antibiotics |
The minimum target group for active trachoma screening should be Indigenous children aged 5–9 years living in communities/towns where trachoma is endemic. |
| |
In communities where trachoma is endemic, annual screening for active trachoma is recommended until active trachoma prevalence is < 5% for 5 consecutive years, after which annual screening should cease. |
| |
All children found to have active trachoma (TF and/or TI) should be treated with single-dose azithromycin |
| |
If ³ 10% of screened Aboriginal and Torres Strait Islander children aged < 10 years have active trachoma and there is no obvious clustering of cases, single-dose azithromycin is recommended for all Aboriginal and Torres Strait Islander children in the community aged 6 months to 14 years and all household contacts aged 6 months or more. |
| |
If ³ 10% of screened Aboriginal and Torres Strait Islander children aged < 10 years have active trachoma and cases are obviously clustered within several households and health staff can easily identify all household contacts of cases, single-dose azithromycina is recommended for all household contacts aged 6 months or more only. Community wide treatment is not required |
| |
If < 10% of screened Aboriginal and Torres Strait Islander children aged < 10 years have active trachoma, single-dose azithromycin is recommended for all household contacts aged 6 months and over |
| |
Antibiotic treatment of cases, household contacts and community members (when required) should be completed within two weeks of screening. |
| |
In regions where population mobility is high, all screening and treatment activities within the region should be completed in as short a timeframe as possible to minimise the likelihood re-infection and to achieve higher population coverage. |
| Facial cleanliness |
Facial cleanliness in children should be promoted by including regular face-washing as part of a holistic personal hygiene program. |
| Environmental health |
Environmental health, school and health promotion staff should be involved as key stakeholders when regional population health units and primary health care services plan and implement trachoma control activities so that ‘F’ and ‘E’ strategies appropriate to individual communities/regions can be implemented. |
Top of page
Acknowledgements
DBM’s work was funded by the Australian Government Department of Health and Ageing on behalf of the Communicable Diseases Network Australia. The authors thank Communicable Diseases Network Australia members and all those who contributed data.
Top of page
References
1. Taylor HR. Trachoma in Australia. Med J Aust 2001;175;371–372.
2. World Health Organization. Primary Health Care Level Management of Trachoma (WHO/PBL/93.33). World Health Organization Programme for the Prevention of Blindness. 1993.
3. Commonwealth of Australia. Specialist Eye Health Guidelines for use in Aboriginal and Torres Strait Islander Populations: Cataract, Diabetic Retinopathy and Trachoma. Canberra (Australia): Office for Aboriginal and Torres Strait Islander Health, Department of Health and Aged Care; 2001. p. 67–95.
4. Francis V, Turner V. Achieving Support for Trachoma Control — A guide for district health work. World Health Organization Programme for the Prevention of Blindness, 1995.
5. World Health Organization. Prevention of Blindness and Deafness — What is Vision 2020? Available from: http://www.who.int/pbd/blindness/vision_2020/en/ Accessed on 7 July 2005.
6. Taylor HR. Trachoma. In: Eye Health in Aboriginal and Torres Strait Islander Communities. Canberra: Commonwealth of Australia; 1997. p. 81–91. Available from: http://www.cera.org.au/new/hrtreview/abts7.html Accessed on 11 February 2005.
7. Mak DV Plant AJTrichiasis in Aboriginal people of the Kimberley region of Western Australia. Clin Experiment Ophthalmol 2001;29:7–11.
8. Thomson N, Paterson B. Eye health of Aboriginal and Torres Strait Islander people. Aboriginal and Torres Strait Islander Health Reviews 1998;1.
9. Western Australian Department of Health. Goldfields Aboriginal Health Plan: A Report for the Regional Planning Team. 1999. Available from: http://www.aboriginal.health.wa.gov.au/htm/publications/2002/regionalplans/goldfields.pdf
10. Western Australia Education Department annual data [received with data from Kimberley Public Health Unit].
11. Commonwealth of Australia. Regional Statistics, Northern Territory, 2002 – ABS catalogue no. 1362.7. Canberra: Australian Bureau of Statistics; 2002.
12. Commonwealth of Australia. Regional Statistics, Northern Territory, 1999 – ABS catalogue no. 1362.7. Canberra: Australian Bureau of Statistics; 1999.
13. Kimberley Population Health Unit. A Kimberley Practice. Trachoma control program guidelines. Broome: Kimberley Population Health Unit; 2004.
14. Tate J. Trichiasis screening project. Kimberley Population Health Unit Bulletin 2004:10–13.
15. Winch J. 1993 trachoma survey at Fitzroy Crossing and surrounding communities. Perth: Marr Mooditj Foundation Inc, 1993.
16. Landers J, Henderson T, Kleinschimdt A, Wu J, Ewald D, Burt B. Prevalence of cictricial trachoma in an Indigenous population of Central Australia: The Central Australia trachopmatous trichiasis study (CATTS), Clin Experiment Ophthalmol 2005;33:142–146.
17. Muller R. Prevalence of acute trachoma and trichiasis in the NT – a historical review, 1983–2003, unpublished paper 2003.
18. Lansingh VC, Weih LM, Keeffe JE, Taylor HR. Assessment of trachoma prevalence in a mobile population in Central Australia. Ophthalmic Epidemiol 2001;8:97–108.
19. Stocks NP, Newland H, Hiller J. The epidemiology of blindness and trachoma in the Anangu Pitjantjatjara of South Australia. Med J Aust 1994;160:751–756.
20. World Health Organization. Report of the 2nd global scientific meeting on trachoma. WHO/PDB/GET 03.1. Geneva, 25–27 August, 2003.
21. Couzos S, Taylor HR. Trachoma. In: Aboriginal Primary Health Care: An Evidence-based Approach, 2nd edn. Melbourne: Oxford University Press; 2003. p. 572–93.
22. Therapeutic Guidelines Limited. Therapeutic Guidelines: Antibiotic, version 12. Melbourne: Therapeutic Guidelines Limited; 2003.
23. Centre for Disease Control Northern Territory. Guidelines for the treatment of trachoma in the Northern Territory. Darwin: Territory Health Services; 1998.
24. Central Australian Rural Practitioners Association. CARPA standard treatment manual, 4th edn. Alice Springs: Central Australian Rural Practitioners Association; 2003.
25. Pilbara Population Health Unit. Trachoma protocol. Port Hedland: Pilbara Population Health Unit; 2004.
26. Midwest and Murchison Population Health Unit. Trachoma protocol. Geraldton: Midwest and Murchison Population Health Unit; 2003.
27. Goldfields Population Health Unit. Trachoma protocol. Kalgoorlie: Goldfields Population Health Unit; 2004.
28. Mabey D, Fraser-Hurt N. Trachoma. Clin Evid 2004;11:880–891.
29. Van Buynder PG, Talbot JM, Graham PJ. Trachoma in Australian aboriginals in the Pilbara. [Letter] Med J Aust 1992;156:811.
30. Courtright P, West SK. Contribution of sex-linked biology and gender roles to disparities with trachoma. Emerg Infect Dis 2004;10:2012–2016.
31. Platt E, Johnson G. Trachoma control program 2001. Kimberley Public Health Bulletin 2002; Feb:13–14.
32. Platt E, Macdonald K. Trachoma control program 2000. Kimberley Public Health Bulletin 2001; Feb:26–27.
33. Wallace T. Trachoma treatment program in the Katherine region. NT Communicable Disease Bulletin 1996;3:13–15.
34. Ewald DP, Hall GV, Franks CC. An evaluation of a SAFE-style trachoma control program in Central Australia. Med J Aust 2003;178:65–68.
35. Yohannes K, Roche P, Blumer C, Spencer J, Milton A, Bunn C, et al. Australia’s notifiable diseases status, 2002: annual report of the National Notifiable Diseases Surveillance System. Commun Dis Intell 2004;28:6–68.
36. Stevens MP, Tabrizi SN, Muller R, Krause V, Garland SM. Characterization of Chlamydia trachomatis opm1 genotypes detected in eye swab samples from remote Australian communities. J Clin Microbiol 2004;42:2501–2507.
37. Communicable Diseases Network Australia. Guidelines for the Public Health Management of Trachoma. Canberra: Commonwealth of Australia; 2006.
38. National Health and Medical Research Council. A Guide to the Development, Implementation and Evaluation of Clinical Practice Guidelines. Canberra: Australian Government Publishing Service; 1998.
39. Emerson PM, Cairncross S, Bailey RL, Mabey DC. Review of the evidence base for the ‘F’ and ‘E’ components of the SAFE strategy for trachoma control. Trop Med Int Health 2000;5:515–527.
40. Mabey D, Fraser-Hurt N. Antibiotics for trachoma (Cochrane review). In: The Cochrane Library, Issue 2, 2004. Chichester, UK: John Wiley & Sons Ltd.
Top of page
Author affiliations
1. Public Health Physician, Communicable Disease Control, Department of Health Western Australia, Shenton Park, Western Australia
2. Associate Professor and Head, Population and Preventive Health, School of Medicine, University of Notre Dame, Fremantle, Western Australia
3. Adjunct Associate Professor, Centre for International Health, Curtin University of Technology, Bentley, Western Australia
4. Policy Officer, Health Strategies Branch, Office for Aboriginal and Torres Strait Islander Health, Department of Health and Ageing, Canberra, Australian Capital Territory
5. Medical Advisor, Health Strategies Branch, Office for Aboriginal and Torres Strait Islander Health, Department of Health and Ageing, Canberra, Australian Capital Territory
6. Director, Primary Care Strategic Policy Section, Primary Care Policy Branch, Primary Care Division, Department of Health and Ageing, Canberra, Australian Capital Territory
Corresponding author: Dr Donna Mak, Communicable Disease Control, Department of Health Western Australia, Grace Vaughn House, 227 Stubbs Terrace, Shenton Park WA 6008. Telephone: +61 8 9388 4828, Facsimile: +61 8 9388 4888. Email: donna.mak@health.wa.gov.au
This report was published in Communicable Diseases Intelligence Vol 30 No 2, June 2006.
